
Laparoscopic partial nephrectomy: The McMaster University
DOI:
https://doi.org/10.5489/cuaj.288Abstract
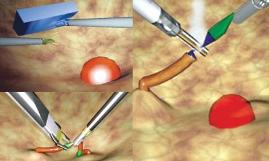
Introduction: Laparoscopic partial nephrectomy (LPN) remains one of the more challenging procedures in urology. Minimizing warm ischemia time (WIT) and bleeding requires efficient intracorporeal suturing. In addition, achieving negative surgical margins requires complete excision of the tumour. We report a large Canadian series of laparoscopic partial nephrectomy with intermediate follow-up.
Methods: Between September 2000 and August 2008, 152 consecutive laparoscopic partial nephrectomies were performed at our centre. Demographic, pathological and clinical data were collected through a retrospective review of the charts.
Results: The average tumour size was 2.68 cm (Range: 0.5-8.8.
The vast majority of tumours were malignant (80%). All margins
were negative, except for 2 patients who underwent an immediate re-resection. There were no local recurrences or distant metastasis during the follow-up period of 44.3 months. Most procedures required hilar clamping (93.4%) with a mean WIT of 34 minutes, with a clear trend for declining WIT with increasing experience. Live procedures were converted to laparoscopic radical nephrectomy, 10 converted to a hand-assisted procedure, and 1 was converted to an open partial nephrectomy. The average blood loss was 162 cc. Complications related to the procedure were classified according to the Clavien grading system. The average drop in the glomerular filtration rate was calculated by the Modification of Diet
in Renal Disease (MDRD) Study equation between preoperative
and 2.5 months postoperative was 8.6 mL/min/1.73 m2.
Conclusions: LPN is a challenging procedure that requires advanced laparoscopic skills. LPN is feasible with excellent oncological outcomes, and an acceptable complication profile. The short-term impact on overall renal function is minimal. The most common postoperative complication was pseudo-aneurysm requiring embolization, which reinforces the intra-operative need for meticulous and a quick suture-ligation of blood vessels during LPN.
Downloads
Downloads
Published
How to Cite
Issue
Section
License
You, the Author(s), assign your copyright in and to the Article to the Canadian Urological Association. This means that you may not, without the prior written permission of the CUA:
- Post the Article on any Web site
- Translate or authorize a translation of the Article
- Copy or otherwise reproduce the Article, in any format, beyond what is permitted under Canadian copyright law, or authorize others to do so
- Copy or otherwise reproduce portions of the Article, including tables and figures, beyond what is permitted under Canadian copyright law, or authorize others to do so.
The CUA encourages use for non-commercial educational purposes and will not unreasonably deny any such permission request.
You retain your moral rights in and to the Article. This means that the CUA may not assert its copyright in such a way that would negatively reflect on your reputation or your right to be associated with the Article.
The CUA also requires you to warrant the following:
- That you are the Author(s) and sole owner(s), that the Article is original and unpublished and that you have not previously assigned copyright or granted a licence to any other third party;
- That all individuals who have made a substantive contribution to the article are acknowledged;
- That the Article does not infringe any proprietary right of any third party and that you have received the permissions necessary to include the work of others in the Article; and
- That the Article does not libel or violate the privacy rights of any third party.

