
Nonstented tubularized incised plate urethroplasty with Y-to-I spongioplasty in non–toilet trained children
DOI:
https://doi.org/10.5489/cuaj.484Abstract
Introduction: This study was designed to evaluate the supportive role of spongioplasty
during tubularized incised plate (TIP) urethroplasty repair of hypospadias.
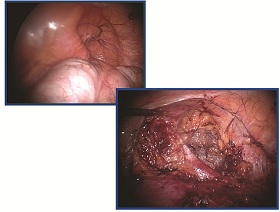
Methods: All non–toilet trained children who underwent TIP repair for primary
hypospadias by 1 surgeon over a 30-month period were included in
our study. The divergent spongiosa was mobilized off the corpora cavernosa
and was rotated toward the midline to wrap the neourethra. A dartos flap
was used to cover the neourethra. The neourethra was calibrated immediately
after surgery in all patients. A urethral stent was left in place only when difficult
calibration was encountered. Complications and cosmetic appearance were
documented at last follow-up.
Results: Thirty-two consecutive patients with a mean age of 18 (standard deviation
[SD] 6) months were included in the study. The defects were distal and
mid-shaft in 26 patients (81.3%) and proximal-shaft in 6 (18.8%). No intraoperative
catheterization difficulties were encountered and all repairs were nonstented.
Antibiotics and anticholinergics were not required. Mean follow-up was
9 (SD 6) months. Urinary extravasation developed in 1 patient (3.1%) on the second
postoperative day. A urethral catheter was easily inserted and left indwelling
for 5 days. One patient presented 6 days postoperatively with suspected voiding
difficulty. Urethral calibration was easily performed excluding any mechanical
obstruction. There were no urinary fistulae and reoperation was not required.
An excellent cosmetic appearance was achieved in all patients.
Conclusion: TIP urethroplasty is a versatile operation that can be performed in
almost all cases of penile hypospadias. A nonstented technique for hypospadias
repair simplifies postoperative care and obviates the need for antibiotics
and anticholinergics. We believe that spongioplasty provides good support
to the neourethra and the hypoplastic distal urethra that may facilitate catheterization
in the immediate and early postoperative periods, if required. Future
controlled study is warranted to further evaluate the role of spongioplasty.
Downloads
Downloads
How to Cite
Issue
Section
License
You, the Author(s), assign your copyright in and to the Article to the Canadian Urological Association. This means that you may not, without the prior written permission of the CUA:
- Post the Article on any Web site
- Translate or authorize a translation of the Article
- Copy or otherwise reproduce the Article, in any format, beyond what is permitted under Canadian copyright law, or authorize others to do so
- Copy or otherwise reproduce portions of the Article, including tables and figures, beyond what is permitted under Canadian copyright law, or authorize others to do so.
The CUA encourages use for non-commercial educational purposes and will not unreasonably deny any such permission request.
You retain your moral rights in and to the Article. This means that the CUA may not assert its copyright in such a way that would negatively reflect on your reputation or your right to be associated with the Article.
The CUA also requires you to warrant the following:
- That you are the Author(s) and sole owner(s), that the Article is original and unpublished and that you have not previously assigned copyright or granted a licence to any other third party;
- That all individuals who have made a substantive contribution to the article are acknowledged;
- That the Article does not infringe any proprietary right of any third party and that you have received the permissions necessary to include the work of others in the Article; and
- That the Article does not libel or violate the privacy rights of any third party.


